Unfortunately, This Winter We Are Not All Cured of COVID-19.
I first heard this theory back in February from a family member: “What if this horrible cold I had this winter was actually COVID-19?” Unlikely, of course, but I wonder what if . But then I started to hear this from more and more people, and now it seems that everyone on Facebook is convinced that they already have coronavirus, they are immune, you can go out, and damn it, we probably all it is already there. …
What a wonderful relief that would be. This will mean that we have already experienced the worst part of the epidemic. His death toll, however large, would have remained in our past. And, perhaps, when the spring flowers bloom, we too will be able to get out of the hiding place – the dark winter of diseases is behind us.
This joyous conclusion should be your first hint that this theory is based more on wishful thinking than fact. The idea just doesn’t add up, so let’s talk about why.
Check where this story comes from
First, and most importantly, this theory does not come from epidemiologists. (Remember, when you have a question about a pandemic, look for people who are subject matter experts , not just those who say what you want to believe.)
Journalist Jane Hu links the recent explosion of these rumors to an article that combined research on immunity from COVID-19 with some unrelated military historian’s speculation. Yes, there are attempts to study how many people may already have acquired immunity to the coronavirus, but they are carried out with the understanding that we are still at the beginning of the virus’s path to the population. In comparison, a recent study found that in the region of Germany most severely affected by COVID-19, with more than 19.0o0 cases, immunity is now only 14% of the population .
There is some truth to rumors that the virus was spreading in secret: many scientists studying the spread of this epidemic actually believe there were more cases than official figures indicate. This is because the US is slow to roll out testing, so many people with COVID-19 are unable to confirm whether they have the virus or not. Even so, they are not rewriting the timeline for when the virus hit the US.
The virus itself tells us where it has been
Coronaviruses don’t have DNA like we do, but they do have something very similar called RNA. Just like you can tell from DNA tests whether your brother is a brother or a half-brother, scientists can analyze viral RNA to see how closely two coronavirus samples are related to each other.
If you contracted COVID-19 from your neighbor, yours and theirs would be nearly identical. Compare your virus to a patient’s virus in another city and it will be clearly related, but with some notable differences. (Viruses accumulate small mutations over time; neither do we, but viruses multiply faster.)
So if you could sequence the viral RNA of each – or even a sample of patients – you could draw a family tree showing how these individual coronavirus samples relate to each other. And since we know when and where each virus appeared in a patient, analyzing the data gives us a pedigree and dates and a map. In fact, there is a massive global project that does just that, called Nextstrain . You can view global data here .
This shows that the earliest Chinese cases were closely related to each other, and the cases that later surfaced around the world were their descendants. There may be gaps in our understanding of the family tree, but it has a clear origin and a clear distribution pattern. “This phylogeny shows an initial appearance in Wuhan, China, in November-December 2019, followed by sustained person-to-person transmission, leading to selective infections,” the website says.
This is confirmed by studies of several groups of scientists. The first two cases in the United States in Washington state were closely related to each other. (This is how public health officials have figured out that the virus is spreading to the public, not just from a few recent travelers.) Two recent analyzes showed that the first cases of New York infection came here via Europe, rather than direct flights from China. …
Data points may be missing and it is likely that some people had undiagnosed cases of COVID in February or even late January. But the big picture is pretty clear: most of us didn’t.
As a result, we do not need to speculate about when and where the virus entered the United States. We have data.
COVID-19 cannot disguise itself as influenza
The data should be enough, but let’s look at the other part of this argument: COVID-19 cases have been dismissed as colds and flu.
There is a rather clear flaw in this logic: COVID-19 is a new disease, and it was discovered because there was a group of patients in China whose symptoms and laboratory tests did not match any known respiratory disease. If cases had started appearing in the United States last fall or early this winter, doctors would have come to a similar conclusion.
New York is now one of the US cities hardest hit by COVID-19. As the virus spread in the city, the number of deaths has skyrocketed. These graphs compare mortality rates (from all causes) in recent weeks versus the previous year and past years. You can’t miss the spike in deaths, hospital cases , and ventilator use . This virus does not go unnoticed.
We have not had an increase in the incidence of influenza either.
Many cold and flu viruses circulate every year. Could mild cases be misdiagnosed? Perhaps several. But not a ton.
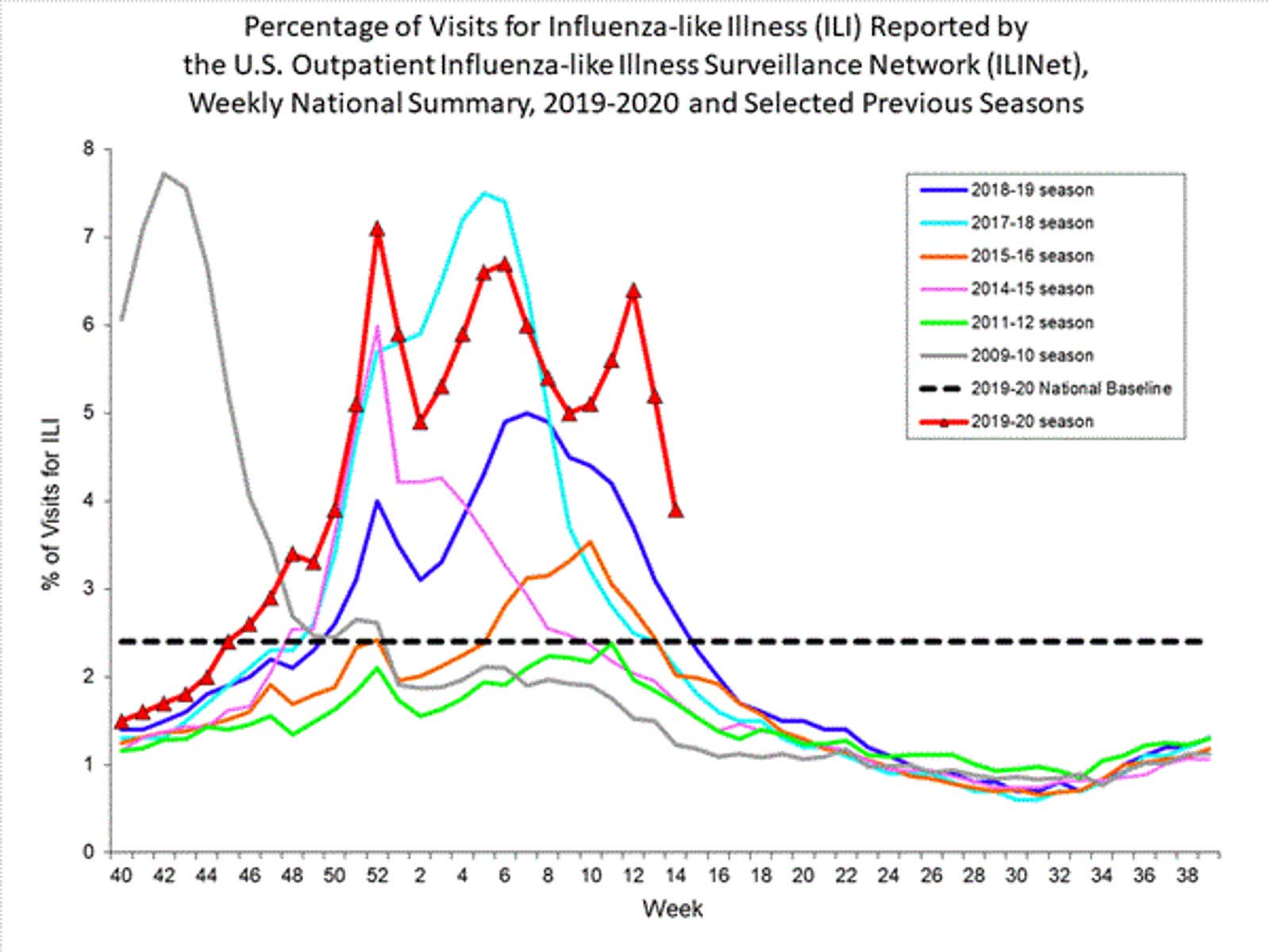
If some colds and flu were indeed COVID-19, there would be no spike in confirmed cases of flu (because they require a positive flu test), but you definitely expect an increase in the number of flu-like illnesses that the CDC is tracking. a project calledILINet . As part of a long-term project, doctors are asked how many patients they visited this week and how many of them had flu symptoms. Specifically: “ILI is defined as fever (temperature 100 ° F [37.8 ° C] or higher) and cough and / or sore throat with no known cause other than the flu.” COVID-19 most commonly presents with fever and cough.
GPP trends this fall and winter are similar to those of previous years. That’s all about this theory.
I know you still want to believe
Think back to the times before the pandemic. Have you ever googled your symptoms and almost convinced yourself that you have a rare disease, or cancer, or something far worse or exotic than what the disease actually turned out to be? Remember, our brains work in strange ways.
Of course, you may have had a worse cold than usual this year. You may have even traveled before you received it. So you are suspicious.
But, again, our brains. Do you remember there was a sniper in Washington ? and the witness said that they saw a white van near the crime scene? After that, other witnesses began to point to the white vans. But everywhere and all the time there are a lot of white vans. Start looking for them; you will see a bunch. It turns out that the white vans had nothing to do with the executions. The snipers were actually flying the blue Chevy .
In this case, colds and flu are white vans. Millions of people get colds or undiagnosed flu every year, so many people have experiences they can mentally associate with COVID-19. So while a handful of people may have had undiagnosed coronavirus infections in February or even late January, the vast majority of your friends’ bad colds this winter were likely just colds.